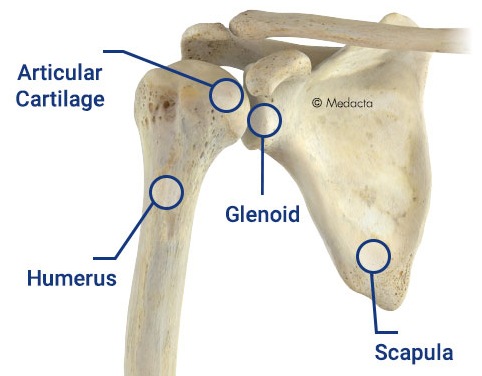
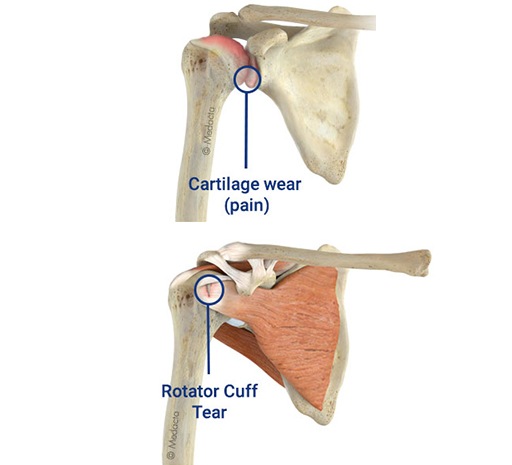
Osteoarthritis of the shoulder is a gradual wearing of the articular cartilage that leads to pain and stiffness. As the joint surface degenerates, the subchondral bone remodels, losing its sphericity and congruity. The joint capsule also becomes thickened, leading to further loss of shoulder rotation. This painful condition is a growing problem in the aging population.
In most cases, diagnosis of degenerative joint disease of the shoulder can be made with careful history, physical examination, and radiography. The symptoms and degree of shoulder arthritis visible on radiography determine the best treatment option.
Mild degenerative joint disease can be treated with physical therapy and over-the-counter anti-inflammatory medications such as acetaminophen or nonsteroidal anti-inflammatory drugs.
More advanced cases of osteoarthritis that are refractory to nonoperative management can be managed with corticosteroid injections. In severe cases, surgery is indicated.
Surgical options include arthroscopic debridement, arthroscopic capsular release, and, in the most severe instances, hemiarthroplasty or total shoulder arthroplasty.